Medicine has always been a profession powered by memory, pattern recognition, and endurance. For decades, the MBBS-to-MD journey rewarded those who could carry entire encyclopaedias of disease in their minds, decode symptoms faster than peers, and survive sleepless nights of clinical grind without losing judgment. That era is now fading—not because doctors are becoming irrelevant, but because the very definition of a doctor is being rewritten by Artificial Intelligence. The stethoscope, once the most sacred emblem of medical authority, is being quietly overshadowed by something far more invisible and powerful: the algorithm.
AI is no longer a futuristic curiosity. It is already triaging patients, summarising radiology notes, drafting discharge summaries, interpreting pathology slides, flagging drug interactions, and predicting outbreaks. In many hospitals, AI is performing tasks that once belonged to junior doctors—only faster, cheaper, and without fatigue. This shift is not incremental. It is structural. Healthcare is no longer merely the science of diagnosis; it is rapidly becoming a system of decision workflows where human judgment must constantly compete with machine confidence.
However, the AI revolution is not uniform. It is shaped by geography, economics, and the particular weaknesses of each healthcare system. In developed systems like the United States, the greatest disease is not shortage of doctors but administrative suffocation. Physicians spend astonishing portions of their day on billing codes, insurance documentation, compliance paperwork, and endless electronic health record rituals. In such an ecosystem, AI does not arrive as a “medical genius.” It arrives as an administrative co-pilot—an attempt to return time to clinicians by automating bureaucracy. In the West, AI is marketed less as a surgeon and more as a liberator: fewer clicks, fewer codes, more time with patients.
India faces a very different battlefield. Here, the crisis is not paperwork—it is scale.
In many public health environments, consultations last two minutes, not because doctors are careless, but because population load makes depth a luxury. The Indian doctor is not trapped by forms; the Indian doctor is trapped by arithmetic. In this reality, AI becomes something else entirely: a scale engine. It acts as multilingual triage, symptom checking, and first-level screening, filtering cases before they reach scarce human attention. As generative models gain fluency in Indian languages, AI begins to promise something radical—transforming healthcare from an urban privilege into a mass-access utility.
This is why India’s AI story is uniquely consequential. India is not building glamorous AI hospitals first; it is building street-level algorithmic medicine. Telemedicine platforms like eSanjeevani offer a foundation for AI integration at scale. Public health programs are experimenting with predictive models and AI-enabled surveillance. Tuberculosis screening through cough-sound analysis is not merely innovation—it is a strategy to convert low-cost data into early diagnosis, bypassing expensive diagnostic bottlenecks. Indigenous cancer screening tools—thermal imaging for breast cancer, smartphone-based oral cancer detection, and deployable community diagnostics—are transforming preventive medicine into something portable, decentralised, and scalable.
Simultaneously, AI is reshaping medicine’s industrial backbone. Drug discovery is being compressed from months into hours in early-stage modelling. Pharmaceutical companies can now explore molecular candidates at speeds no human research team can match. This is not a small upgrade; it is the compression of scientific time itself. At the same time, hospitals and medical devices becoming digitally connected have created a new medical frontline: cybersecurity. AI is increasingly deployed as a defence layer, monitoring anomalies and intrusion attempts. Yet the paradox is brutal—the most vulnerable systems are often the least replaceable. Legacy scanners, outdated monitoring devices, and ageing hospital servers remain the weakest links, especially in public hospitals. The future of medicine may be algorithmic, but its infrastructure remains painfully analogue.
Yet the most disruptive impact of AI is not technological. It is professional.
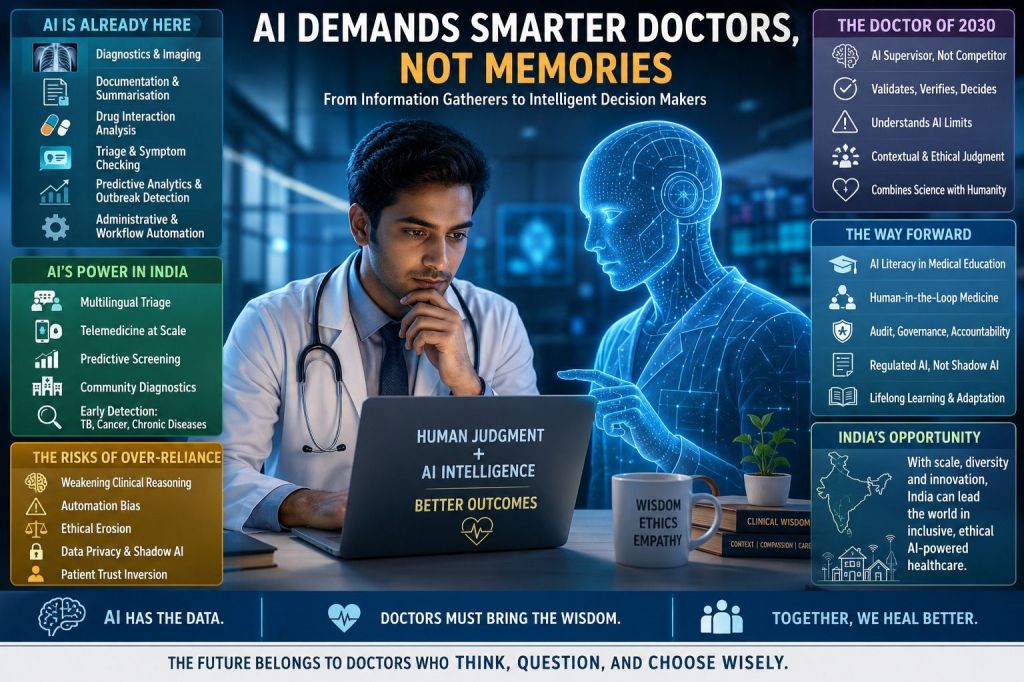
The traditional medical education model was built for a world where recall was the ultimate advantage. Students memorised syndromes, pharmacology, and diagnostic pathways because the human brain was the fastest database available. That logic collapses when AI becomes a better database than any intern. It can recall rare diseases instantly, interpret imaging faster than a junior resident, and draft treatment plans in seconds. This does not mean MBBS or MD degrees are losing value. It means the un-augmented doctor is becoming obsolete.
Medicine is shifting from “information gatherer” to “AI supervisor.” A doctor who competes with AI in routine diagnosis will lose. A doctor who understands where AI fails—hallucinations, bias, missing context, inability to read nuance, and dangerous overconfidence—will remain indispensable. The future belongs to clinicians who can validate machine output, catch errors, and apply judgment in the zones where medicine stops being computation and becomes human art.

This transition creates a unique risk for millennial medical professionals. They were trained in the old world, overloaded in the present world, and now expected to master a new layer of digital competence while exhausted. Late adoption becomes professional erosion. But an even darker threat is emerging among younger doctors: “never-skilling.” If AI solves every diagnostic puzzle during training, the brain never develops the muscle of independent clinical reasoning.
Cognitive offloading becomes silent decay. Over-reliance on AI weakens differential diagnosis instincts. Automation bias—the tendency to trust machine output simply because it sounds confident—can kill patients. Studies already suggest many clinicians fail to detect errors in AI-generated communications because the output looks polished and authoritative. The machine speaks fluently, so the human stops questioning. Even moral deskilling becomes a danger. If AI recommends an “efficient” treatment pathway, will the doctor recognise when efficiency conflicts with what is ethically best for the patient? If the doctor becomes an algorithm’s employee, ethics becomes a checkbox.

A parallel crisis is already unfolding: shadow AI. Physicians are increasingly using consumer-grade AI tools informally for drafting, summarisation, and decision support. Yet many hospitals lack governance frameworks. Sensitive patient data risks being processed through systems that do not meet privacy standards. In India, where regulation is still evolving, this creates a delayed scandal waiting to erupt—data leaks, malpractice disputes, and institutional failures that will arrive suddenly, long after the habit becomes normalised.
Even trust is being redesigned. Patients now arrive with lab reports “explained” by AI. If the doctor disagrees, the patient may distrust the human. At the same time, the doctor may trust the AI too much. This produces a strange inversion: the patient becomes suspicious of human judgment, while the clinician becomes dependent on machine confidence. Healthcare begins to resemble a courtroom where the doctor must argue against an algorithm that speaks with perfect certainty.
Medical education is not keeping pace. Curricula still reward memorisation rather than algorithmic supervision. Residency programs rarely provide structured training in AI literacy, bias detection, or verification discipline. Worse, poorly designed hospital AI systems can increase burnout instead of reducing it—adding friction, workflow complexity, and more digital burdens.
The way forward is not rejection. It is disciplined integration. The winning model is human-in-the-loop medicine: clinicians must reason independently first, then use AI as a comparator, not as a master. AI outputs must be logged, audited, and discussed. Hospitals must establish clear acceptable-use policies distinguishing approved embedded systems from dangerous shadow usage. Licensing systems must eventually treat AI literacy not as a luxury skill, but as a patient safety requirement.
India’s opportunity is immense. With its scale and multilingual complexity, Indian doctors who master AI translation, triage, and remote chronic monitoring will gain unmatched leverage. The doctor of the future will not only treat patients, but orchestrate digital tools to extend care into villages, reduce diagnostic delays, and personalise health education in local languages.
AI will not replace doctors. But it will absolutely replace doctors who refuse to evolve. The doctor of 2030 will not be the one with the best memory. It will be the one with the sharpest judgment—because in a world where intelligence is everywhere, wisdom remains the rarest medicine.
VISIT ARJASRIAKNTH.IN FOR MORE INSIGHTS
