India debates inequality with obsessive passion—income inequality, caste inequality, gender inequality, rural-urban inequality. Every budget speech contains at least one paragraph on inclusion. Every policy document is coated in the language of empowerment, dignity, and access. Yet one of the most brutal forms of deprivation remains almost entirely invisible, precisely because it does not show up in balance sheets or fiscal deficit calculations. It does not appear in poverty ratios or GDP graphs. It appears in queues. It appears in the hours lost outside hospitals, ration shops, transport offices, police stations, municipal counters, and government portals that promise “seamless service” while quietly manufacturing delay.

This is temporal inequality: the unequal distribution of time as a cost of survival. For the affluent, time is elastic. It can be purchased, outsourced, and monetized. A wealthy citizen can pay for convenience, book appointments, access private healthcare, hire agents, use premium delivery services, and navigate digital platforms with ease. Even bureaucratic friction becomes a negotiable inconvenience. But for the poor, time is not money. It is life itself—traded daily for wages, food, caregiving, and dignity. Every hour spent waiting is not a mild inconvenience. It is an hour stolen from income, health, sleep, and the fragile arithmetic of survival. In India, the poor do not just earn less. They also wait more.
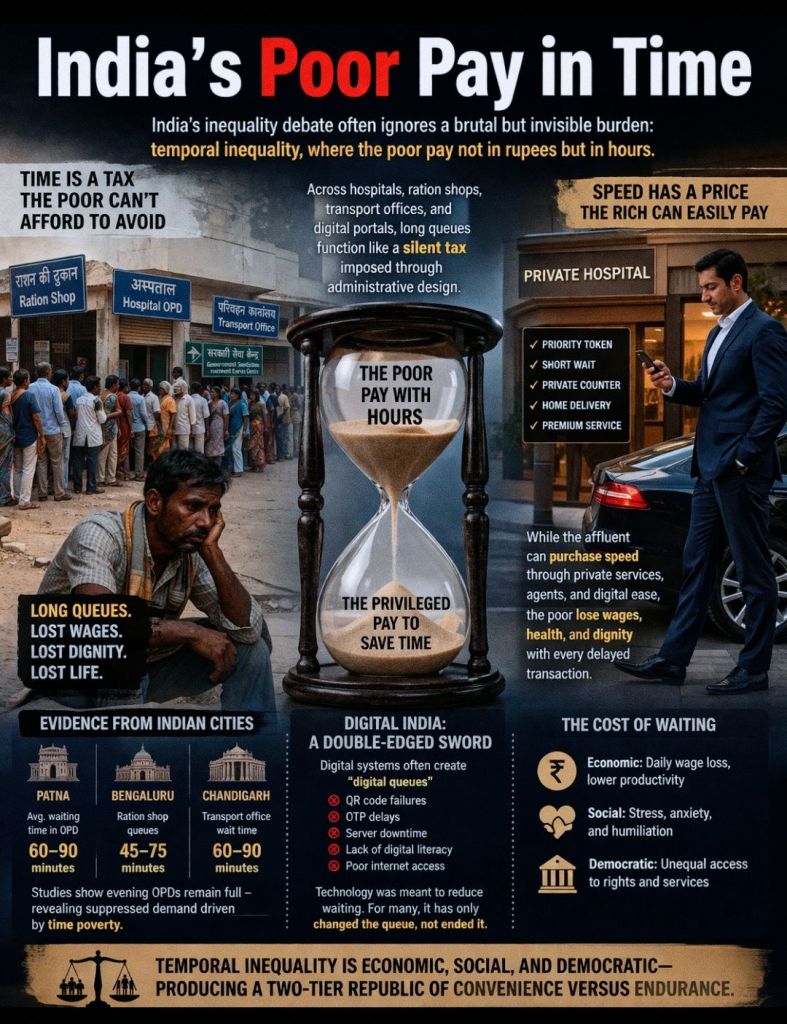
Temporal inequality is therefore not a soft sociological concept. It is a hard economic and political fact. It functions like a silent tax—imposed not by legislation, but by administrative design. Unlike monetary poverty, time poverty cannot be recovered later. A missed day’s wage cannot always be compensated. A delayed diagnosis cannot be reversed. A lost day spent chasing signatures is not merely wasted time; it is a slow erosion of agency. The poor are not only underpaid. They are systematically over-delayed.

This is why temporal inequality produces what sociologists call a hierarchy of belonging. The privileged citizen experiences the city as responsive, navigable, and negotiable. The poor citizen experiences the city as delayed, uncertain, humiliating, and exhausting. Citizenship is not only a constitutional status; it is also temporal access—the right to be served without losing half one’s life in the process. In that sense, the Indian state does not merely distribute welfare. It distributes waiting.
And waiting is not an exception. It is the operating system. Consider public hospitals in Patna. Average waiting times range between 60 and 90 minutes. PMCH records 75–85 minutes, AIIMS Patna around 90 minutes, and IGIMS—handling 7,000 to 7,500 patients daily—forces patients into queues of 60–70 minutes. Bihar’s rural average touches 80 minutes. Meanwhile, Katihar district reports just 29 minutes, proving that long waits are not inevitable. They are not fate. They are often the predictable result of overload, poor design, and administrative indifference. Waiting time is governance quality made visible.

Bengaluru reveals an even sharper cruelty. Elderly patients reportedly wait 90 minutes merely to obtain registration tokens at Namma Clinics. QR-based registration systems and ABHA-linked authentication create digital queues, but those without smartphones or digital literacy are forced into a second layer of waiting: waiting to access the queue itself. Many seniors struggle with OTP authentication, adding 15–20 minutes per transaction. For a poor elderly citizen, even a basic consultation becomes a marathon. Modernity arrives as a screen, but access is still rationed by literacy, device ownership, and bandwidth. The state calls it “digital empowerment.” The citizen experiences it as digital exhaustion.

Chandigarh’s experience provides an even clearer diagnosis. GMSH-16 receives 3,500 OPD patients daily within a narrow morning window. When an evening OPD pilot was introduced in February 2026, 395 patients arrived in six days. This was not random footfall. It was suppressed demand—citizens who could not afford to lose wages during the day finally found time-accessible healthcare. Nearly 30% of evening OPD patients came for medicine consultations, suggesting something profound: people were not avoiding care because they were healthy, but because they were time-poor. Healthcare was not inaccessible only due to money; it was inaccessible because of time.
Then came the great promise that was supposed to end this humiliation: Digital India. Digital governance was marketed as the great equalizer. Remove middlemen, reduce corruption, accelerate service delivery, reduce waiting. But across sectors, digital systems have often produced the opposite effect. They have created a new architecture of exclusion—one that does not abolish waiting, but relocates it into digital bottlenecks while multiplying barriers for those with limited access.
This is the digital queue paradox: technology does not eliminate waiting; it reorganizes it. Smartphone dependency is the first trap. QR-based systems assume device ownership, stable internet, data packs, and familiarity with apps. But millions still use basic phones or share devices within families. The result is predictable: those who cannot register digitally must stand aside, seek assistance, and lose time even before entering the formal process. The queue now begins outside the queue. The poor must first prove they deserve to stand in line.

OTP authentication becomes the second trap. A system designed for security becomes a time penalty for the elderly, visually impaired, and digitally unfamiliar. ABHA frameworks may be visionary on paper, but on the ground they become procedural mazes when failed OTPs, repeated logins, and multiple-step verification dominate the experience. The poor are not resisting technology; they are being defeated by it. The state calls it “paperless.” The citizen experiences it as paperwork without paper.The third trap is infrastructure inequality. Despite the expansion of Common Service Centres, persistent issues remain: unreliable connectivity, power interruptions, weak rollout of services, low digital literacy, and corruption that adapts rather than disappears. Digitization, without capacity-building, becomes a sophisticated gatekeeping machine. The counter has not vanished. It has simply migrated into a portal.

The Lancet Commission’s citizen survey across 50,000 households confirms this pattern: access has expanded, but delivery assurance remains weak due to governance gaps and uneven district-level capacity. In other words, platforms may exist, but functioning service ecosystems often do not. India built the website, but not the reliability. It built the app, but not the doctor. It built the dashboard, but not the queue discipline. Temporal inequality is not accidental. It is produced by structure. The first driver is chronic underinvestment. Public health spending remains below 2% of GDP, while insurance schemes focus heavily on hospitalization rather than OPD, diagnostics, and medicines—the very services that generate the longest queues. The poor wait because free services are under-resourced.

The second driver is geographic concentration. Tertiary hospitals in cities like Patna serve entire states. IGIMS receives volumes far beyond its design capacity. Rural PHCs may have shorter queues but lack specialists, forcing referrals to overcrowded urban hubs. The poor do not travel because they want better care; they travel because the system funnels them into collapse zones. The third driver is workforce shortage and broken referral systems. Digital registration cannot create doctors. Apps cannot manufacture nurses. QR codes cannot expand hospital wards. Technology cannot substitute for staffing.
For daily wage workers, a 90-minute wait is not a delay. It is a wage cut. Multiple visits for certificates, ration disputes, hospital follow-ups, and transport documentation create compounded income loss. The poor therefore delay care until emergencies, further overloading emergency departments and deepening system collapse. This becomes a vicious cycle: the poor wait longer, lose income, delay services, fall sicker, and then require costlier interventions. Waiting becomes both cause and consequence of poverty.
Digital governance adds an even deeper political dimension. Those with time can research policies, question governance, file RTIs, attend hearings, and participate in democracy. Those trapped in survival queues often cannot. Temporal inequality is therefore not only economic; it is democratic. It silently manufactures a two-tier republic: one class with time to live and decide, another class with time only to endure. India does not lack solutions. Chandigarh’s e-Sampark model shows assisted digital systems reduce multiple visits. Punjab’s faceless transport system shows how doorstep delivery reduces repeated travel. Katihar’s efficiency proves management reforms can outperform sheer spending. International models sharpen the lesson: Estonia’s integrated digital identity prevents repeated paperwork; Rwanda’s WhatsApp-based triage works even on basic phones; Brazil integrates telemedicine with primary care; the UK enforces maximum wait standards.
The strategic shift required is simple but revolutionary: India must stop measuring success in digital transactions and start measuring success in minutes saved for the poorest citizen. Temporal inequality is perhaps the most humiliating form of deprivation because it consumes life silently. The poor are not only economically disadvantaged; they are forced to surrender time, wages, health, and dignity in exchange for services that should be rights. If India wants to build a modern welfare state, it must recognize that governance is not only about schemes and portals. Governance is also about queues. And until the Republic reduces the waiting time of its poorest citizens, India’s digital transformation will remain incomplete—not because technology failed, but because equity was never made the design principle.
VISIT ARJASRIKANTH.IN FOR MORE INSIGHTS
